J Pediatr Endocrinol Metab 2025; aop
Letter to the Editor
Pankaj Prasun* and Rebecca C. Pulvermacher
ANKS1B is a potential candidate gene for short
stature and failure to thrive in children
https://doi.org/10.1515/jpem-2025-0295
Received May 26, 2025; accepted August 18, 2025;
published online August 27, 2025
Abstract: Short stature and failure to thrive are among the
most common reasons for referral to pediatric endocrinologists. The etiology could be endocrine, genetic, nutritional,
psychological, or a systemic disease. Genetic syndromes account for about 5 % of short stature in childhood. However,
with increased use of genomic technologies in clinical diagnosis, the number of genes associated with short stature and
failure to thrive is increasing. Some of the genetic syndromes
such as Silver–Russell syndrome is clinically recognizable,
while others may present as isolated short stature. We
recently found ANKS1B intragenic deletion in a child with
short stature, failure to thrive, and subtle distinct physical
features, who was referred to us for evaluation of Silver–
Russell or other genetic syndromes associated with short
stature. ANKS1B is associated with neurodevelopmental disorders. However, animal study and genetic association
studies suggest its role in somatic growth as well. Our observations suggest that ANKS1B is a potential candidate gene for
short stature and failure to thrive in children.
Keywords: ANKS1B; genetic short stature; failure to thrive;
Silver–Russell syndrome
Short stature and failure to thrive in childhood are common
referrals to pediatric endocrinologists. The majority of
children with short stature are healthy and have isolated
short stature. It is usually either familial or a constitutional
delay of growth. Short stature when associated with failure
to thrive is concerning for a genetic syndrome, hormonal,
nutritional or psychological disorder, or a chronic systemic
disease. Accurate diagnosis is crucial for proper management and adequate outcome. With routine use of genomic
*Corresponding author: Pankaj Prasun, MD, Department of Pediatrics,
Division of Genetics, American Family Children’s Hospital Madison,
Madison, USA, E-mail: [email protected]. https://orcid.org/0000-00025949-6421
Rebecca C. Pulvermacher, Department of Pediatrics, Division of Genetics,
American Family Children’s Hospital Madison, Madison, USA
technologies in clinical practice, understanding of the genetics of short stature and failure to thrive is expanding.
While many genetic syndromes are clinically recognizable,
some genetic conditions may present with isolated short
stature, which would have otherwise been diagnosed as
idiopathic short stature. For example, heterozygous hypomorphic pathogenic variations in SHOX, IGF1, IGF1R, and
FGFR3 have been associated with isolated short stature [1].
We have found heterozygous ANKS1B intragenic deletion in
a child with short stature and failure to thrive who was
referred for evaluation of Silver–Russell syndrome.
This individual, a 6-year-old male, was born at 39-week
gestation via cesarean section. Antenatal, birth, and
neonatal periods were uncomplicated. His birth weight was
3,220 g m (29th centile), length 48.3 cm (26th centile), and
head circumference 35 cm (34th centile). During infancy, he
was noted to be fussy with food and “would spit up a lot.” He
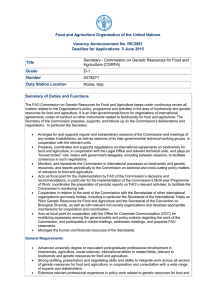
was diagnosed with lactose intolerance, but the feeding issues persisted on lactose-free diet. His weight fell off to 3rd
centile at 9 months and 1st centile (Z score – 2.27) at
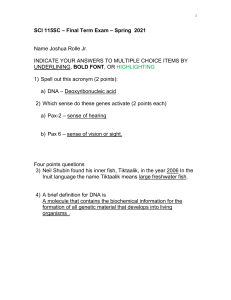
15 months of age (supplementary Figure 1). His height fell off
from 21st centile at 2 years of age to 3rd centile at 3 years of
age and below 1st centile (Z-score – 2.49) at 4 years of age
(supplementary Figure 2). He was diagnosed with asthma as
a toddler. His appetite would decrease significantly during
the frequent asthma attacks precipitated by upper respiratory tract infections. The patient attained developmental
milestones mostly on time. There was concern for gross
motor delays, but he caught up without the need of any
supportive therapy. Significant behavioral and sensory issues were noted in early childhood. He was very sensitive to
noise and change in environment and would make selfsoothing body rocking movements when seated. He was
diagnosed with stereotypic movement disorder and anxiety.
The patient was evaluated by a neuropsychologist at 4 years
of age due to these concerns. A formal diagnosis of sensory
processing disorder was made. The neuropsychologist
thought that he might have high functioning autism spectrum disorder. He is doing well academically.
The patient was evaluated by a pediatric gastroenterologist at 5 years of age for poor weight gain. Celiac disease and
other malabsorption syndromes were ruled out. Difficulty in
2
Prasun and Pulvermacher: ANKS1B and failure to thrive
gaining weight was initially attributed to frequent asthma
attacks and poor calorie intake during those episodes. He was
prescribed cyproheptadine, which improved appetite but
poor weight gain persisted. Subsequently, nutritional deficiency was considered unlikely explanation of his failure to
thrive. He was evaluated by a pediatric endocrinologist at
5 years of age. His bone age was consistent with chronological
age. Constitutional or familial short stature was considered
unlikely. Growth hormone deficiency was ruled out. The short
stature was proportionate, and there was no body asymmetry. However, he was noted to have subtle facial features
reminiscent of Silver–Russell syndrome; hence, referral to
genetics for evaluation of genetic syndromes associated with
short stature was made.
The patient was evaluated in genetics clinic at 5 years
and 4 months of age. On examination, his weight was
13.2 kg (<1 centile, Z-score - 3.44), length 100.1 cm (1st centile, Z-score −2.30), and head circumference 49.2 cm (5th
centile, Z-score – 1.6). Frontal prominence with prominent
veins, triangular facies, pointed small chin, high arched
palate, and bilateral clinodactyly of fifth finger were noted.
Silver–Russell syndrome was considered unlikely as he did
not meet the Netchine–Harbison clinical scoring system
(NH-CSS) criteria. Moreover, methylation and highresolution copy number variation assays for Silver–Russell syndrome were normal. Chromosome microarray
showed a 106 kb deletion on chromosome 12q23.1 [arr
[GRCh37]12q23.1 (100087407_100192972) x1]. This is an
intragenic deletion involving exons 5–8 of ANKS1B. Deletion of similar size in this region has been reported before
to cause ANKS1B haploinsufficiency [2, 3]. Parental studies
showed that this deletion was maternally inherited. This
individual’s mother does not have short stature or history
of failure to thrive in childhood. Hence, trio exome
sequencing (proband and parents) was obtained to rule out
other possible genetic etiologies. It revealed a paternally
inherited pathogenic variation, c.7689 G>A (p.W2563 *) in
FLG encoding filaggrin associated with ichthyosis vulgaris
and atopic dermatitis [4]. No other significant finding was
reported.
ANKS1B encodes for AIDA-1 (amyloid precursor protein
intracellular domain associated-1). AIDA-1 is highly
expressed in brain [2]. Intragenic deletions in ANKS1B are
associated with a spectrum of neurodevelopmental disorder
including autism spectrum disorder, attention deficit hyperactivity disorder, and speech and motor deficit [2].
Intragenic deletions in ANKS1B are very rare, but often
inherited from one of the parents who may be unaffected or
mildly affected implying reduced penetrance and variable
expressivity [2]. It has not been reported with short stature
or failure to thrive in childhood thus far. However, mice that
were heterozygous for anks1b deletion showed significant
decrease in weight, length, and brain size [2]. Interestingly,
this difference was sex-specific as only male mice showed
significant growth impairment. This could explain why the
patient’s mother is unaffected even though this deletion is
maternally inherited. Genome wide studies have shown association of ANKS1B polymorphisms with body mass index
[5, 6]. Moreover, the ANKS1B interactome analysis showed
major role in organismal development apart from nervous
system development and function [2]. Although, the patient
does not have cognitive impairment, there are significant
social and behavioral concerns such as sensory processing
disorder, anxiety disorder, and a suspicion of high functioning autism spectrum disorder. A recent animal study has
demonstrated that Anks1b deficiency leads to deficits in social behavior and sensory reactivity [7]. Apart from the
ANKS1B intragenic deletion, this individual was also found
to have pathogenic variation in FLG associated with childhood atopic diseases including early-onset asthma [8].
Although, it may explain his dairy intolerance and earlyonset asthma, short stature and failure to thrive appear
directly related to the ANKS1B haploinsufficiency.
We have described here an individual with ANKS1B
intragenic deletion presenting with short stature and failure
to thrive. Although the causality is not proven, there are
multiple lines of evidences suggesting role of ANKS1B in somatic growth apart from its previously known role in neurodevelopment. ANKS1B haploinsufficiency should be
suspected when growth impairment is associated with neurodevelopmental and/or neurobehavioral concerns. Subtle
but distinct physical features such as those resembling Silver–
Russell syndrome (prominent forehead, triangular facies,
clinodactyly) seen in the individual described here or round
facies, midfacial hypoplasia, brachycephaly, astigmatism, and
brachydactyly described in other individuals with ANKS1B
microdeletion may provide further clue [2].
In conclusion, our clinical observations support ANKS1B
as a potential candidate gene for short stature and failure to
thrive. More clinical/basic science data are needed to
establish a causative role of ANKS1B haploinsufficiency in
short stature and failure to thrive of childhood.
Research ethics: Not applicable.
Informed consent: Informed consent was obtained from all
individuals included in this study, or their legal guardians
or wards.
Author contributions: All authors have accepted responsibility for the entire content of this manuscript and
approved its submission. Dr. Pankaj Prasun prepared the
manuscript, was involved in patient care, laboratory interpretation, and genetic counseling. Rebecca C Pulvermacher
Prasun and Pulvermacher: ANKS1B and failure to thrive
was involved in patient care, laboratory interpretation, genetic counseling, and revised the manuscript.
Use of Large Language Models, AI and Machine Learning
Tools: None declared.
Conflict of interest: The authors state no conflict of interest.
Research funding: None declared.
Data availability: Not applicable.
References
1. Jee YH, Andrade AC, Baron J, Nilsson O. Genetics of short stature.
Endocrinol Metab Clin N Am. 2017; 46:259-81.
2. Carbonell AU, Cho CH, Tindi JO, Counts PA, Bates JC, ErdjumentBromage H, et al. Haploinsufficiency in the ANKS1B gene encoding AIDA1 leads to a neurodevelopmental syndrome. Nat Commun. 2019; 10:
3529.
3. Foreman J, Perrett D, Mazaika E, Hunt SE, Ware JS, Firth HV. DECIPHER:
improving genetic diagnosis through dynamic integration of genomic
and clinical data. Annu Rev Genom Hum Genet 2023; 24:151-76.
3
4. Smith FJ, Irvine AD, Terron-Kwiatkowski A, Sandilands A, Campbell LE,
Zhao Y, et al. Loss-of-function mutations in the gene encoding filaggrin
cause ichthyosis vulgaris. Nat Genet. 2006; 38:337-42.
5. Croteau-Chonka DC, Marvelle AF, Lange EM, Lee NR, Adair LS, Lange LA,
et al. Genome-wide association study of anthropometric traits and
evidence of interactions with age and study year in Filipino women.
Obesity. 2011; 19:1019-27.
6. Lee SI, Kim SK, Kang SW. Genetic variants associated with body mass
index changes in Korean adults: the anseong and ansan cohorts of the
Korean genome and epidemiology study. Curr Issues Mol Biol. 2024; 46:
9074-81.
7. Cho CH, Deyneko IV, Cordova-Martinez D, Vazquez J, Maguire AS, Diaz JR,
et al. ANKS1B encoded AIDA-1 regulates social behaviors by controlling
oligodendrocyte function. Nat Commun. 2023; 14:8499.
8. Bønnelykke K, Pipper CB, Tavendale R, Palmer CN, Bisgaard H.
Filaggrin gene variants and atopic diseases in early childhood
assessed longitudinally from birth. Pediatr Allergy Immunol. 2010; 21:
954-61.
Supplementary Material: This article contains supplementary material
(https://doi.org/10.1515/jpem-2025-0295).
 0
0