Murfreesboro City Schools Please be sure to read all instructions
Anuncio

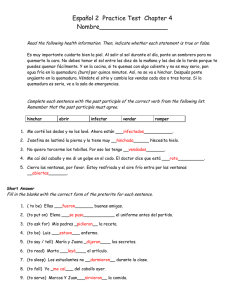
Murfreesboro City Schools Ruth Bowdoin Preschool Program Thank you for your interest in the Murfreesboro City Schools Preschool Program. We are excited about the coming year. Our preschool classrooms will be located in several schools for the 2015-2016 school year. The school locations for the classrooms are tentative and will depend on space available. We will continue to offer classrooms at our off site locations at Mercury Court, Oakland Court and Franklin Heights. Children who reside within the Murfreesboro city limits and meet the eligibility requirements, regardless of your child’s zoned school, may be placed in a classroom based on location, zones, and proximity as long as space is available. At this time all PreK classrooms are fully enrolled. However, we are accepting applications for the waiting list as openings do occur. Please turn in completed forms with required documentation at the Murfreesboro City Schools Central Office after August 8th between the hours of 8:00 and 4:00. If a qualifying space becomes available, you will be contacted at that time. If you have questions, you may contact us by email at [email protected]. INSTRUCTIONS FOR APPLYING FOR PREK Please be sure to read all instructions carefully and bring all appropriate documentation when you return your application. Your child must be 4 years old on or before August 15, 2015. You must live within the city limits of Murfreesboro and be zoned for a Murfreesboro City School. Completing the application: *If you are downloading to print from the website there will 6 pages* 1) The Application should be filled out front and back. All information must be complete for the application to be considered. Don’t forget to sign and date at the bottom of page 2. 2) The Income Eligibility Form must be completed for your application to be considered. Be sure you list ALL individuals that live in your household in Part A. Part B should be completed if you or your child participates in any of these programs. You must have official documentation and case numbers to verify your participation in these programs. Be sure to bring that documentation with you when you return your application. This information MUST be officially verified. Be sure to sign on the back page of this form. Part C is to be completed ONLY if you did not check any box in Part B. Read the instructions for Part C carefully. Income for all family and household members must be listed. Income verification documentation as listed in the box MUST be brought when you return your application. *** Be sure to check the boxes for the documentation you are providing for Part B or C When you return your Application you must bring the following : We will be keeping all the documentation. Please bring COPIES, not originals of bills, birth certificate, social security card, and income documentation. Completed Application and Income Eligibility forms Proof of your address. The only documentation that will be accepted is copy of an electric, water, or gas bill with the parent’s name and the service address on it. These bills may be no more than 60 days old. If you do not pay these bills, you must have a copy of your official lease in the parent/guardian’s name. • Copy of Official Birth Certificate (not a mother’s copy). If your child was born in Tennessee, a birth certificate may be obtained at the Rutherford County Health Department. • Copy of your child’s Social Security card * Copy of appropriate documentation to verify the information you provided on the Income Eligibility form from either Part B or Part C. This documentation should include either your DHS letter confirming your child’s enrollment in a public assistance program like food stamps or Families First. If you do not receive public assistance, we require verification of income. You may bring your 2014 W2 or 1040 or 1040A tax return. • • * All applicants will be considered for additional services or slots provided or funded by partnering agencies, therefore, we ask that you submit a W-2 or 2014 tax return in addition to state required documents (or other supporting documents). Submitting these will expedite the processing of applications. Why we require documentation to support your application: *Only children who are 4yrs. old, but not yet 5, by Aug. 15, 2015 are eligible. A birth certificate is the only documentation recognized by the state. *Only children who live within the city limits of Murfreesboro are eligible for the program. A utility bill, electric/gas/water, issued within the last 60 days are the only documents accepted. If you do not pay utilities, we require a copy of a current lease. *In addition we require information on your family income. Please see the information below excerpted from the website of the TN Dept. of Education: Enrollment in the Voluntary Pre-K program is based upon a child’s eligibility as identified in TCA 49-6101─104. Available space in each school system is limited and is based on the funding awarded each year through a grant process. Enrollment Priority Requirements Pursuant to state law 49-6-101: priority is given to students identified as economically disadvantaged/ low income. This identification is based on income levels set each year by the Department of Health and Human Services and used during the application process to determine income eligibility for enrollment. OFFICE USE ONLY DOB CK_________________________ Address CK______________________ Zone__________________________ Murfreesboro City Schools Preschool Program ( A Partner with Mid-Cumberland Head Start ) APPLICATION MUST BE COMPLETE AND ACCURATE TO BE CONSIDERED Child’s Name as it appears on the birth certificate: ______________________________________________________________________ First Middle Last Date of Birth ______________ Sex_____ Race______ Phone #___________________ Social Security # ____________________ Language Spoken at Home______________ List any special needs____________________________________________________ Does your child live with (circle all that apply): Mother Father Grandparents Guardian Is your child able to handle toileting habits independently: (circle one) Yes No Mother/Guardian Information Name ________________________________ Phone ( ) -_____ - _________ Address______________________________________________ Zip Code__________ Place of Work____________________________ Work phone_____________________ Father/ Guardian Information Name _______________________________ Phone ( ) - ______ -__________ Address________________________________________________ Zip Code________ Place of Work____________________________ Work phone_____________________ Parent Email address ______________________________________________________ Extended School Program (ESP): Will your child need extended childcare? ________My child will not need ESP OR My child will need care:____Morning only ____ Afternoon only ____Morning and Afternoon Siblings currently attending Murfreesboro City Schools: Name____________________________________Grade_________School_________________ Name____________________________________Grade_________School_________________ Name____________________________________Grade_________School_________________ Are any siblings currently on an approved zone waiver for the above listed schools. YES or NO Additional Contact Information: Name_________________________ Phone________________ Relationship___________ Name_________________________ Phone________________ Relationship___________ Name_________________________ Phone________________ Relationship___________ Health Information- Please complete carefully and check ALL that apply: _____Allergies? List: ___________________________________________________________ What happens? __________________________ Is Epi-pen prescribed? Circle: Y or N _____Asthma? Is Inhaler used? Circle: Y or N If yes, how often?________________________ What medications are taken for Asthma? ____________________________________________ _____Diabetes? Circle: Type I or Type II What medications are taken? ____________________ _____Special procedures? Describe ________________________________________________ _____ADD or ADHD? What medications are prescribed? _______________________________ Will medication be taken at school? Y or N When? ______________________________ _____Seizures? What type? _________________ Date of last seizure ____________________ Is Diastat prescribed? Y or N What other medications are prescribed? ______________ _____Episode of loss of consciousness? When? _____________________________________ List any other medical problems or concerns which you would like the school to know about: _____________________________________________________________________________ Student’s Doctor______________________________________ Phone____________________ Student’s Specialist___________________________________ Phone ____________________ Student’s Dentist______________________________________ Please contact the school for Medication or Procedure Forms if your child requires medication or procedures during the school day. I understand that I am required to provide transportation to and from preschool for my child every day. I have read the instructions for the application process and understand that I must provide all necessary documentation for my child’s application to be considered. I agree to comply with all regulations and policies of the Murfreesboro City Preschool Program. I understand that I may be contacted by MidCumberland Head Start for selection into a partnership slot. I give my permission for Murfreesboro City Schools to verify any information on the application, including income. I understand that acceptance into this school is contingent upon my city residency. If I move outside the city limits during the school year, my child will no longer be allowed to attend the preschool. I understand that unacceptable attendance may be grounds for removal from the program. ________________________________________________________________ Parent/Legal Guardian’s Name (print) ________________________________________________________________ Parent/Legal Guardian’s Signature date TN Department of Education Office of Early Learning-­‐ Corrected 2015 US Health and Human Services Poverty Guidelines *Annual income levels reflect 185% of the 2014 US Health and Human Services Poverty Guidelines, equivalent to reduced priced lunch criteria. Household Size 1 2 *Annual Income $21,775.00 $29,471.00 Monthly $1,815.00 $2,456.00 Twice per Month $908.00 $1,228.00 Every two weeks $838.00 $1,134.00 Weekly $419.00 $567.00 3 $37,167.00 $3,098.00 $1,549.00 $1,430.00 $715.00 4 $44,863.00 $3,739.00 $1,870.00 $1,726.00 $863.00 5 $52,559.00 $4,380.00 $2,190.00 $2,022.00 $1,011.00 6 $60,255.00 $5,022.00 $2,511.00 $2,318.00 $1,159.00 7 $67,951.00 $5,663.00 $2,832.00 $2,614.00 $1,307.00 8 $75,647.00 $6,304.00 $3,152.00 $2,910.00 $1,455.00 For each additional person, add $7,696.00 $642.00 $321.00 $296.00 $148.00 This chart is to be used when reviewing the Pre-­‐K Income Eligibility application to determine if family meets income qualifications for "economically disadvantaged." Families making at or below the annual income amount, based on household size, meet the income eligibility criteria for participation in the Voluntary Pre-­‐K program for the 2015-­‐16 school year. Verification must include total income of all household family members as indicated on Pre-­‐K income THIS CHART MAY NOT BE USED FOR ELIGIBILITY FOR FREE or REDUCED PRICED LUNCH PROGRAM. Meeting Income eligibility requirements does not guarantee acceptance into the VPK program due to limited space and the possibility of more students applying than seats available. For Office Use Only Please Circle One Income Eligible: Yes / No 2015-16 Application to Determine Income Eligibility for the Voluntary Pre-K Program Completion of this form DOES NOT qualify your child for the Free or Reduced Meal Program. application is not a guarantee of acceptance into the VPK program. Name of Student: Date of Application: SSN of Student: Date of Birth of Student: Name of Applicant: Relationship to Student: Submission of this Mailing Address: City: State: Home Phone #: ( Work Phone #: ) ( Zip Code: Cell Phone #: ) ( ) Part A - Family Information Please list information for all other household members. Section 1 Name(s) of ALL OTHER CHILDREN in the Household Date of Birth School Grade 1. 2. 3. 4. 5. Section 2 Name(s) of ALL OTHER ADULTS in the Household Relationship to Student 1. 2. 3. 4. 5. Total # of household members: Part B - Program Participation Please check (√) if Child /Family /Household member provides documentation of participation, in one or more of the following programs, currently or during past school year (*Documentation required-See Part D). (√) (√) (√) Early Head Start Foster Care Head Start Homeless (√) Migrant Case # Families First (TANF) Food Stamps / EBT Siblings met eligibility for Free or Reduced Price Meal Program in 2014-2015 *If submitting proof of qualifying for any of the above programs, you do NOT need to complete Part C. Updated: January 31, 2014Feb 27,2015 ED-5476 Division of Special Populations Part C - Total Household Income Please list ALL INCOME of all household family members and how often income is received. Any falsification of information concerning income, residence, birth certificate and/or completion of this application and other forms may be reason for dismissal. Income Instructions From the list below, please write the Source of Income Code in the space provided to indicate the source(s) of income for each earning individual in the household. Also, please write the Monthly Payment or Wage Amount. Multiply the Payment or Wage amount by the number months you received the income and then calculate the Amount and the Total Annual Income. Source of Income Codes A. GROSS work income D. Pension(s) G. Veteran's Benefits J. SSI Disability B. Unemployment E. Retirement H. Child Support K. Other - please list C. Workman's Comp F. Social Security I. Alimony Name of Adult Employer (if applicable) Source of Income Code (See list above) Monthly Payment or Wage Amount $ - Multiplied by (X) ↓ How many months did you receive this income in the last year? Total Amount X $ - $ - X $ - $ - X $ - $ - X $ - $ - X $ - Total Annual (Yearly) Income $ - Part D - INCOME VERIFICATION Please check (√) all documents submitted as Proof of Income or Program Participation. Pay Stub / Verification of pay by employer Retirement Documentation Foster Care Reimbursement W-2 Form Social Security SSI Documentation Income Tax Form 1040A or 1040 Veteran's Benefit Letter TANF Documentation Unemployment Compensation Child Support AFDC / Public Assistance Payment Workman's Compensation Documentation Alimony Documentation TennCare Verification Pension Stubs Other (Specify): → I certify that the above information in this application is correct. I further understand that any falsification of information concerning income, residence, birth certificate and/or completion of this application and other forms may be reason for dismissal from Tennessee's Voluntary Pre-K Program. Printed Name of Applicant: SSN #: Signature of Applicant: Date: Name and Signature of LEA employee reviewing this application I certify that I have examined the above income documentation and verification information. forms must be maintained in accordance with FERPA. Completed Printed Name / Title of LEA employee: Signature of LEA employee: Date Reviewed by LEA employee: Updated: January 31, 2014Feb 27,2015 ED-5476 Division of Special Populations Solo para uso oficial Please Circle One Income Eligible: Yes / No 2015-16 La solicitud para decidir la elegibilidad de los ingresos para la investigación preescolar voluntaria Rellenar este impreso NO resulta en la clasificación del estudiante para comidas escolares gratis y a precio reducido. Nombre del Estudiante: Fecha: Número del Seguro Social de la Estudiante: Fecha de Nacimiento: (mes/día/año) Nombre en letre de molde del solicitante o de uno de los padres: Relación a estudiante (padre/madre) Direccion: Ciudad: Estado: Teléfono de su casa: ( Codigo Postal: Teléfono de su trabajo: ) ( Numero cellular: ) ( ) Parte A - Información de la Familia Por favor, lista información sobre su familia Sección 1 Nombres de otro niños en su casa: Fecha de Nacimiento Nombre de Escuela Grado 1. 2. 3. 4. 5. Sección 2 Nombres de otros adultos en la casa: Relación a estudiante (por ejemplo: padre/madre): 1. 2. 3. 4. 5. Cuantas personas que viven en la casa: Parte B - participación en el programa Por favor, marca (√) si su hijo/a o su familia participa en uno de esos programas (la documentación) (√) (√) (√) Early Head Start Foster Care Head Start Sin Hogar (√) Migratorio Case # Families First (TANF) Food Stamps / EBT Los hermanos del estudiante reciben comida gratis o precio reducio en la escuela (NSLP) en 2014-15. Si presenta documentación de las programas como se dice más arriba, no es necesario completar Parte C. Updated: February 27, 2015 ED-5476 Division of Special Populations Parte C - Suma de Ingresos de Hogar Por favor, lista TODOS LOS INGRESOS de la familia y con qué frecuencia recibe. Falsificacion de la informacion de ingreso, residencia, o otro preguntas resulta en dimisión de la investigación. Ingreso Instrucciones De la lista debaja, por favor escriba El Codigo de los Ingresos en el espacio e indique el tipo de ingreso recibe. Tambien, por favor escriba el suma en un mes y multiplica de el numbero de meses que recibe este typo de ingreso. Calcula el total por un año. Codigo de los Ingresos A. Ingreso del trabajo D. Pension(es) G. Beneficios de Veteranos J. Ingresos del seguro de discapacidad B. Cheque for desempleo? E. El fundo de retiro H. Manutencion de los hijos K. Otro - por favor, lista C. Compensacion al Trabajadore F. Seguro Social? I. Alimentos Nombre de Adulto Empleador (si aplicable) Codigo de Ingresos Multiplica de: Pago en un mes Cuantos meses usted recibe este ingreso ↓ Suma $ - X $ - $ - X $ - $ - X $ - $ - X $ - $ - X $ - Suma de Ingresos en un año $ - Parte D - Verificación de los Ingresos Por favor marca (√) todos que has presentado en sus comprobantes de ingreso. Talon de pago/verificacion de empleador Retiro Documentacion Cuidado de crianza documentacion W-2 Forma Seguro Social SSI Documentacion Income Tax Forma 1040A or 1040 Letra de los Veteranos TANF Documetacion Desempleo Forma Manutencion de los hijos AFDC / Public Assistance Payment Documentación de Compensacion al Trabajadore Documentación de los Alimentos TN Care Verificacion Pension(es) Otro (Lista): → Certifico que toda la información en esta solicitud es verdadera y correcta. Entiendo que falsifico intencionalmente de los ingeresos o la dirección puede resulta in dimisión de la programa Pre-K. Nombre en letre de molde del solicitante: SSN #: Firma de solicitante: Fecha: Sólo por uso oficial. No escribe debajo de esta linea. Name and Signature of LEA employee reviewing this application I certify that I have examined the above income documentation and verification information. forms must be maintained in accordance with FERPA. Completed Printed Name / Title of LEA employee: Signature of LEA employee: Date Reviewed by LEA employee: Updated: February 27, 2015 ED-5476 Division of Special Populations